

Foundational Paper 002 - The invisible infrastructure that decides whether your child gets sick this week
A daycare with hundreds of children was spending the same on cleaning as an average household. This is what we found about why hygiene systems fail in silence.

Key Points
Cleaning was never housekeeping. It is public health infrastructure. And like all infrastructure, it fails in silence.
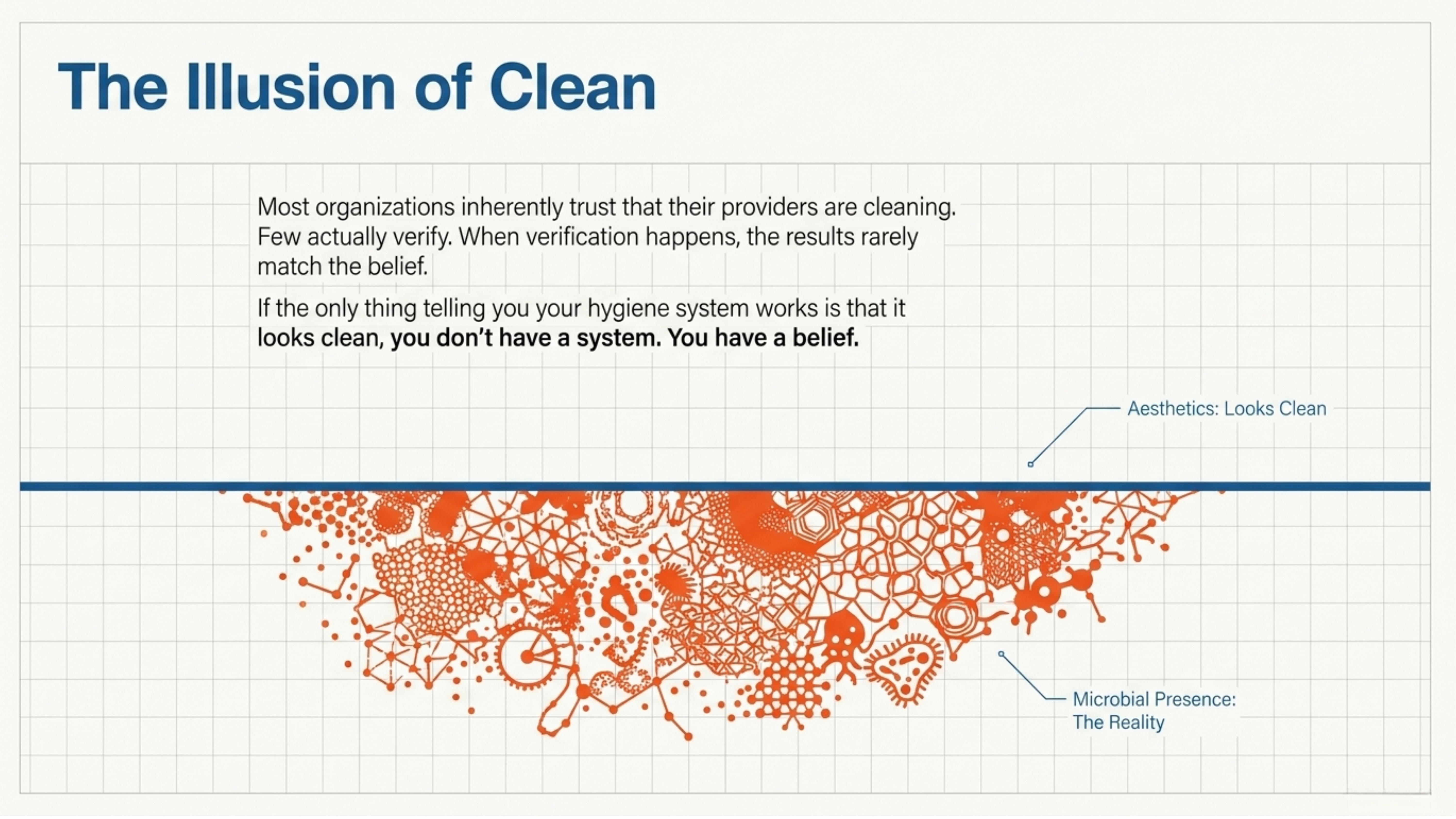
If the only thing telling you your hygiene system works is that it looks clean, you don’t have a system. You have a belief.
Hygiene systems fail where responsibility gets diluted.
What isn’t designed on purpose ends up designed by default.
The cost is paid by whoever has the least voice in the decision.
👋 Hi, it’s Luisa Javier. Welcome to Aziul Connections (🌎🔬 The Sustainable Systems Lab), where I study how sustainable systems are built for business, leadership, and life.

🎧 Listen to Luisa read this article
A daycare with hundreds of children and a household-sized budget
Some time ago, an educational institution caring for hundreds of children reached out to the WAYAKIT team. They wanted a quote on cleaning products. When we reviewed their monthly spend, we found something that stayed with me for several days. They were spending on cleaning roughly what an average household spends.
They weren’t the only one. We have prospected several daycares and schools, and this pattern shows up more often than I would like. It’s not conscious negligence either. What happens with these institutions is what happens whenever a system isn’t designed. It is simply inherited.
What keeps bringing me back to this scene isn’t the number itself. It’s what the number indicates. If an institution caring for hundreds of children is cleaning on a household budget, we are likely talking about an institution cleaning with water. And the parents of those children don’t know.
This is the thesis I want to open today:
Cleaning was never housekeeping. It is public health infrastructure. And like all infrastructure, it fails in silence.
What we call infrastructure, and what we don’t
When someone says public health infrastructure, we picture hospitals. Vaccines. Drinking water networks. Things with plaques, public budgets, ribbon-cutting ceremonies.
Everyday hygiene is also infrastructure. What happens day after day in a daycare, in an aircraft cabin, in a hotel room, in a restaurant kitchen. But we don’t see it that way. We don’t fund it that way. We don’t audit it that way.
An international group of experts led by Matthew Freeman and Jonny Crocker met in Dakar and last year published a paper in Nature Water worth bringing into this conversation. They argue that hygiene interventions at scale have failed to sustain real change because we think of them as standalone products or as campaigns, when in reality they are hygiene systems that need design, maintenance, metrics, and redesign.
Katelyn Jetelina, the epidemiologist behind Your Local Epidemiologist (also published in Spanish as Su Epidemiólogo Local, translated by Dr. Maria Zoco), articulated it a few weeks ago with an image that sticks: public health is an invisible shield. It works quietly in the background, preventing crises we never see. And there lies the design problem. If no one sees it, no one feels it, no one can define it, no one sustains it.
What I learned measuring the invisible
Five years of my doctorate at KAUST were spent measuring ATP on desalination membranes with a lab luminometer. ATP is adenosine triphosphate, the energy molecule of every living cell. When you measure ATP on a surface, you are not counting specific bacteria. You are measuring whether microbial life is present. It’s a fast proxy, imperfect, but brutal in its honesty: the cleaning method worked or it didn’t.
Today we have moved that same measurement into the field, now with portable equipment. Aircraft cabins. Hotel rooms. Trays, seatbelts, remote controls, touchscreens. The measurement happens in situ, before and after applying the existing cleaning protocol. What we see breaks the assumption.
The constant: most organizations trust that their providers are cleaning. Few verify. And when verification happens, the results don’t match the belief.
And this pattern isn’t regional. It is documented globally. In Brazilian hospitals, hand hygiene compliance averages 47%. In a study measuring prevalence across hospitals in Brazil, Venezuela, Mexico, and Colombia, one in ten hospitalized patients had at least one healthcare-associated infection (12.26% regional average, Mexico 13.24%). At Mexico’s Hospital Infantil Federico Gómez, implementing an automated hand hygiene monitoring system reduced infections by 43.4 to 56.7 percent.
A line worth marking:
If the only thing telling you your hygiene system works is that it looks clean, you don’t have a system. You have a belief.
Where responsibility gets diluted
There is a design pattern sustaining this problem, and it’s worth naming. Hygiene systems fail where responsibility gets diluted.
Parents trust the daycare. The daycare trusts its provider. The provider delivers what was asked of them, almost always at the lowest possible price. And still, children get sick more than they should. A CDC analysis documented that 22% of households of daycare caregivers experience secondary transmission of diarrheal disease. The figure is from 2004 and hasn’t improved enough. Infections that happen inside the daycare end up in the homes, in the siblings, in the grandparents.
Lindsay Dahl, the environmental health lobbyist behind The Environmental Health Brief, names it precisely in a recent essay: there’s a story we tell ourselves about toxic products that goes something like this. The problem is in your home, and the solution is now your personal burden. Swap the pan, filter the water, replace the couch. Her argument is that this narrative is not accidental. It is structural, and the real solution doesn’t live in the individual consumer but in public policy and systems design. Her work focuses on chemical policy, but the principle applies to hygiene more broadly. When the regulatory or institutional system fails, the cost gets transferred to the end user, who almost never has the information or the power to solve it.
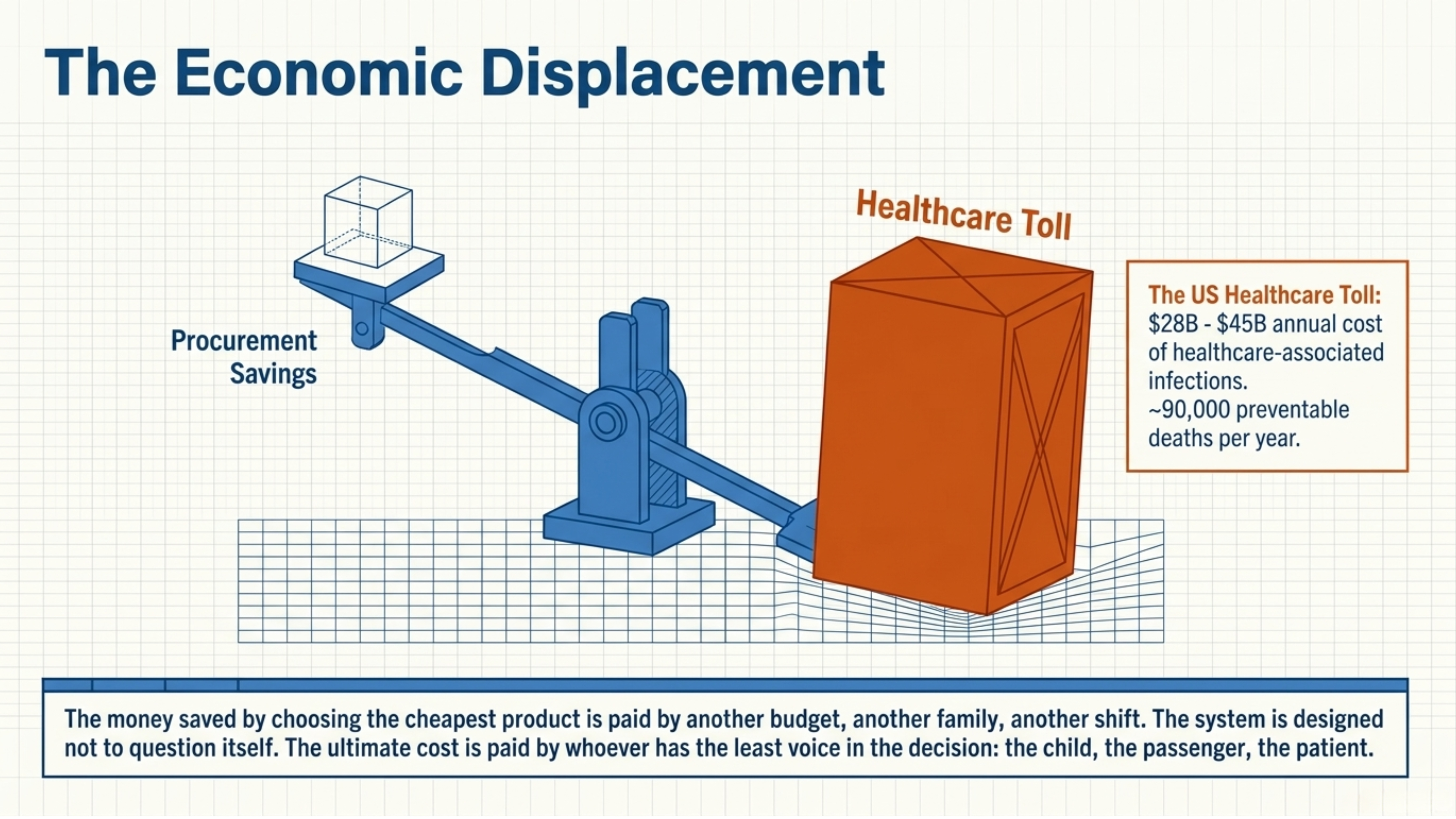
There are three specific reasons the system fails in silence. The first is metric. Almost no one measures ATP outside the lab, and what isn’t measured doesn’t enter the operational conversation. The second is the product label. That phrase about killing 99.9% of germs sounds sufficient until you understand against which pathogens. There are viruses that don’t fit trivially in that remaining 0.1%, and the products that inactivate them are different from the ones that kill common bacteria, a technical distinction that almost never reaches procurement. The third is cost. In the United States alone, healthcare-associated infections cost between 28 and 45 billion dollars per year and kill approximately ninety thousand people, most of them preventable. The money procurement saved by choosing the cheapest product is paid by another budget, another family, another shift.
And this is where the system gives itself away. What I am describing is not individual negligence. It is a system designed not to question itself.
The cost is paid by whoever has the least voice in the decision: the child in the daycare, the passenger on the flight, the patient in the hospital bed.
The question no one is asking
I want to come back to the daycare for a moment. Not to resolve it, but to reopen the question.
When I was the mother of a baby boy, many years ago now, it didn’t occur to me to ask. I didn’t have this information. I didn’t have this knowledge. I trusted, the way parents trust their daycares right now, the way passengers trust airlines, the way patients trust hospitals.
Hygiene is public health infrastructure. What isn’t designed on purpose ends up designed by default. By default means: by lowest price, by habit, by blind trust.
The next time you walk into a space where others trust it is clean, it’s worth asking who is measuring what, and who pays if no one is watching. This is not about distrust. It is about applying to hygiene the same logic you would apply to any other critical infrastructure.
In the next pieces of this series, we are going to open the box. What is actually being measured, against what reference, why the products you think are protecting you aren’t always doing it, and what questions are worth starting to ask now, before someone else gets sick.
Subscribe to Aziul Connections (The Sustainable Systems Lab)
Public lab studying sustainable systems across business, leadership, and life. Essays, experiments, field observations and case studies from a climate-tech founder (Dr. Luisa Javier) operating between LATAM and MENA. Aziul = Azul (the planet) + Luisa (backwards)
About the author: Dr. Luisa Javier
Dr. Luisa Javier is a scientist and climate-tech entrepreneur across LATAM and MENA, focused on designing sustainable systems for business and society. She is the Founder and CEO of WAYAKIT Group and the author of Aziul Connections.
Aziul Connections is the public lab where I study how sustainable systems are built.
“I build sustainable living through WAYAKIT, and study the systems behind it through Aziul Connections.”
Thank you for reading or listening to this article. Share it or leave a comment if you found this information useful.
Luisa
References
Freeman, M. C., Crocker, J., et al. (2025). Systems thinking for hygiene: an interdisciplinary approach to sustained behavior change. Nature Water. https://www.nature.com/articles/s44221-025-00424-9
Jetelina, K. (2026). Happy Public Health Week. Your Local Epidemiologist (Substack).

Su Epidemiólogo Local — Spanish-language edition of Your Local Epidemiologist, translated by Dr. Maria Zoco.
Telles, J. P., et al. (2025). Hand hygiene compliance in Brazilian hospitals. The Lancet Regional Health – Americas (via PubMed Central). https://pmc.ncbi.nlm.nih.gov/articles/PMC11875181/
Huerta-Gutiérrez, R., et al. (2019). Prevalence of healthcare-associated infections in Latin America. International Journal of Infectious Diseases (IJID). https://www.ijidonline.com/article/S1201-9712(19)30261-9/fulltext
Salinas-Escudero, G., et al. (2023). Impact of an automated hand hygiene monitoring system on healthcare-associated infections at Hospital Infantil de México Federico Gómez. Frontiers in Public Health. https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2023.1117680/full
Centers for Disease Control and Prevention (CDC). (2004). Diarrheal illness in children attending child care. Emerging Infectious Diseases. https://wwwnc.cdc.gov/eid/article/10/11/04-0623_04_article
Dahl, L. (2026). Care about the environment, but dismiss toxic chemicals in products as pseudoscience? Read this. The Environmental Health Brief (Substack).
Stone, P. W. (2009). Economic burden of healthcare-associated infections: an American perspective. Expert Review of Pharmacoeconomics & Outcomes Research (via PubMed Central). https://pmc.ncbi.nlm.nih.gov/articles/PMC2827870/
WAYAKIT Group. Corporate site.
https://sa.wayakit.com
King Abdullah University of Science and Technology (KAUST).
https://kaust.edu.sa
Note on currency: References #7 (CDC, 2004) and #9 (Stone, 2009) are older sources, kept here because they remain the canonical studies cited in subsequent literature. The specific figures may have shifted in magnitude, but the documented pattern still holds.